
Developing oral drugs for antibody targets
A differentiated fast-follower strategy for the bold

Protagonist and J&J recently achieved a major milestone by delivering a Phase 3 oral psoriasis treatment that matches the mechanism of Tremfya—a blockbuster antibody with over $3 billion in annual sales. Patients can now consider a once-daily pill instead of frequent injections, a huge win for biopharma and healthcare alike.
Here, we’ll explore the value of developing oral drugs for antibody targets, the business considerations at play, and the technical ingenuity required to design such molecules.
The case for developing these drugs
Oral drugs still set the bar for patient convenience, it’s simply tough to get easier than a once-daily pill. On the contrary, think about the inconvenience involved in IV infusions for your typical antibody drugs - scheduled clinic visits, infusion chairs, and trained healthcare staff. Subcutaneous (SubQ) injections is an improvement, but it still requires cold-storage and self-injections.
Few other advantages worth highlighting:
Patients at mild or early-stages of disease may be reluctant to begin injection-based therapies but open to oral drugs given the minimal lifestyle disruption. Part of this is also driven by the societal view that patients requiring injections are perceived as more sick. This means that an oral drug can drive earlier adoption & overall improved outcomes
Oral drugs can be more easily co-administered without other oral drugs in a combo setting
Antibody drugs have a long half-life, which is problematic if the patient turns out to have an adverse event. The short half-life of an oral drug is an advantage
Oral drugs don’t require cold storage or infusion centers, making global distribution easier
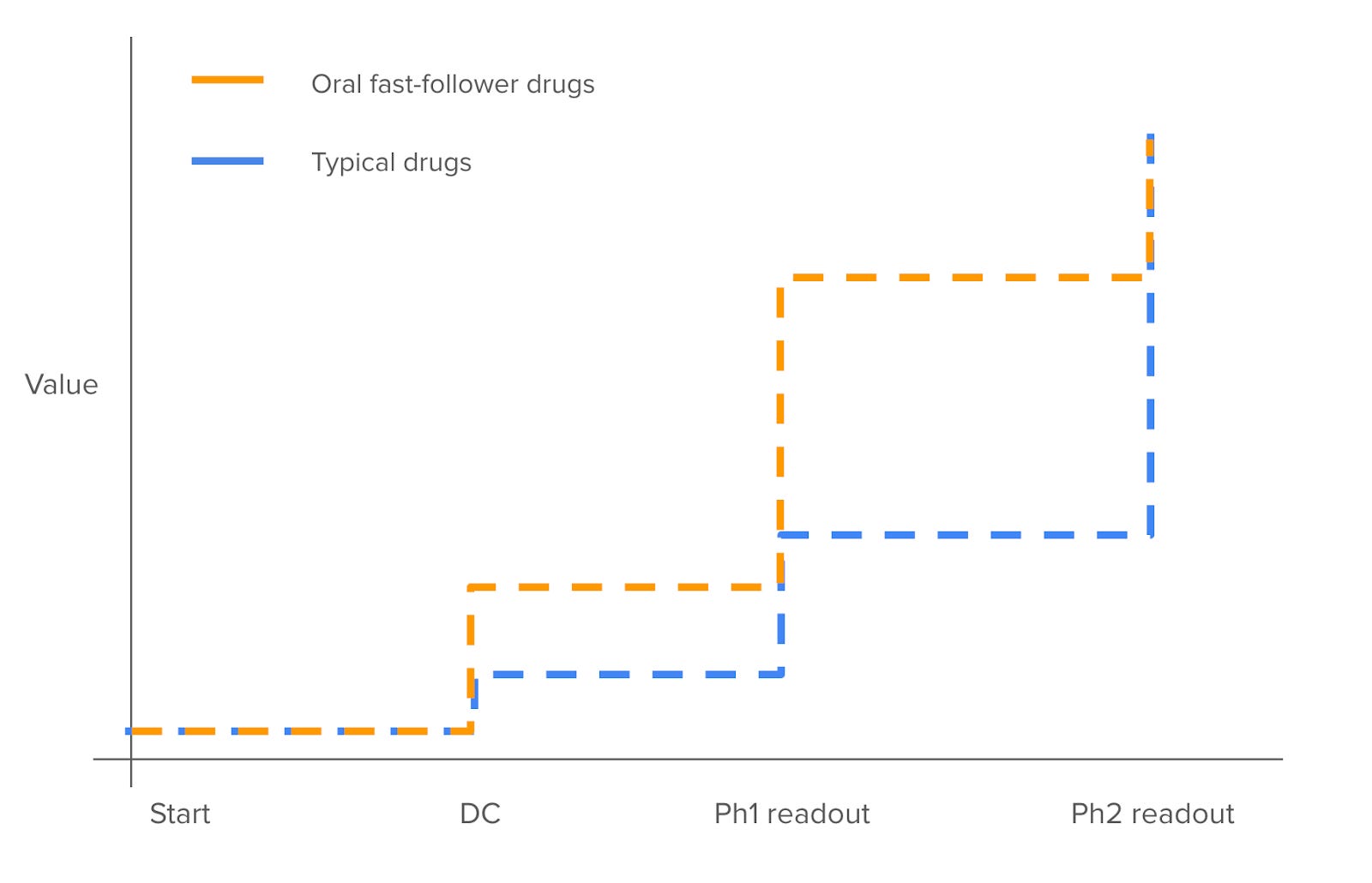
For biotechs in this space, the inflection points arrive earlier
Typically in biotech, the key inflection point for any drug (or company) is the Phase 2 readout since it shows whether the drug is efficacious. Phase 1 safety readout is somewhat derisking, but rarely a meaningful value-creating event.
But in the case of oral drugs for antibody targets, value creation happens much earlier.
Developing the preclinical drug itself gives the company a lot of credit. That’s because designing a good molecule is often very difficult for reasons we’ll discuss later, and the existing antibody already derisks much of the clinical and market risk.
Phase 1 in healthy volunteers is particularly important for these companies, because the PK/PD data is highly informative. The existing antibody that has gone through trials already informs us what PD markers matter for the desired clinical profile. Therefore, reasonable PK data to enable oral dosing and also demonstrate PD markers at parity (or improvement) to the existing drug already derisks much of the future clinical profile of the drug, thereby creating value. For instance, Morphic’s a4b7 drug showed ~100% receptor occupancy at 100mg BID, which gave comfort and excitement for many investors.
This is a great perk - in a world where value creation can take a long time, companies in this space can generate value rather quickly once it enters clinical trials.
But designing these drugs are challenging from a scientific standpoint
There’s no free lunch in biopharma - if the market and biology is derisked, it must mean that engineering these molecules is quite difficult. Here’s what I mean.
Let’s first define the risks:
Biological risk: will hitting this target in this fashion lead to the desired clinical profile?
Engineering risk: how hard is it to design the said molecule?
Market risk: if this drug achieves the desired clinical profile, will it sell?
You’re always trading off one type of risk for another. If a drug has low biological and engineering risk, it likely has substantial market risk given the competition from many other me-toos. You can reduce that competitive risk by going earlier than others, but now you’re taking biological risk since there is not yet validation. When a target is obvious but there’s no competitors, you can assume that developing the right candidate takes immense engineering work (e.g. KRAS g12c, Myc).
So why are building oral drugs for antibody targets hard?
Antibodies typically inhibit a target by disrupting its native interactions with other proteins, but it’s difficult for a small molecule to disrupt that same protein-protein interaction (PPI). The interface is often flat and smooth, unlike the pockets and cavities that small molecules conventionally address. It’s like how a rock climber can easily ascend a rugged cliff filled with cracks and protrusions they can grab onto, while they would struggle with a smooth wall.
The key insight is that interactions in PPI are not all created equal, but rather certain “hot spot” residues contribute a substantial amount of the binding energy. That means a small molecule approach can focus on these energetically significant hotspots instead of covering the whole surface. At times, this may even map to a compact, druggable pocket. An example is Tirofiban which targets αIIbβ3, which interacts with fibrinogen through the RGD motif that creates a 300–500 Ų sized pocket for a RGD motif mimetic to drug.
Many of the success cases have been peptide-like drugs, which makes sense since the peptide of the interaction domain is the most straightforward starting point. Examples of these peptidomimetics are Venetoclax, Nutlins, the Smac mimetics, Bromodomain inhibitors like JQ1 that mimic peptides but are small molecule-like.
Macrocycles have been particularly effective for this target class. They have peptide-like properties and can bind large surfaces with tertiary interactions, which makes it more suitable for disrupting PPIs than typical small molecules. Designing these drugs though is still more art than a science, especially since you have to balance its desired PD properties with the need to make it orally available and metabolically stable. The oral bioavailability has been a tough nut to crack, especially our current preclinical assays like Caco-2 and PAMPA aren’t so reliable. That being said, I’m optimistic that the ongoing advances in mRNA display library and computational chemistry tools will make this process easier.
The business challenges in building these companies and ways to mitigate them
So given that designing these drugs is difficult and can take long timelines, how does one operationalize this as a company? These startups often need at least two rounds of financing to go from idea to DC. That’s because the necessary capital would be too large for a single round (with the exception of a strong fundraiser or if you’re starting with a good hit), or the campaign just took longer than initially planned for. This means that the second financing will need to be raised with a molecule still in development, which can be challenging at times. The other challenge is that any single campaign is quite risky.
Another risk is that a new mechanism that raises the bar for the field can emerge. Of course this risk is universal for any biotech program, but it particularly applies for these strategies since the oral drug would be entering the clinic several years after the existing antibody product hit PoC, giving several years for new innovation to occur. So it’s worth mitigating this risk by simultaneously pursuing multiple scaffolds on the same target or developing drugs for other targets. This, of course, means more capital intensity.
These challenges are why having a central platform story can be valuable. First, the sheen of the platform can help raise equity capital that can go into your campaign. Second, the technology can command non-dilutive capital through collaboration with pharma, a strategy that DICE / Protagonist / Morphic used effectively. Finally, and perhaps most importantly, the platform can help you develop that drug. Indeed, DICE’s DEL screen got them their initial hits for their IL-17 program. A broad technology that can improve the oral bioavailability of a complex molecule could also help.
What to expect next
These are tough drugs to build but handsomely rewarding when done right - I’m excited to see additional companies pursuing this strategy. Three questions that came to mind as I put this together:
The new wave of long-acting antibodies (e.g. Spyre, Apogee) could enable Q3M and Q6M SubQ dosing frequency. How will oral drugs match up against these? I’m curious to see how adoption plays out. Morphic vs. Spyre would be an interesting battleground to watch if they’re both approved.
Approved antibodies will eventually go off patent and biosimilars will enter the market, eroding pricing power even for the oral equivalent drugs. Would this meaningfully disincentivize the desire to develop that drug? So far, biosimilar entry & adoption has been painfully difficult but this could change.
Is this strategy an implicit bet against innovation? To believe that the oral equivalent of the established antibody to be successful, you also have to believe there won’t be a novel mechanism that meaningfully advances on efficacy/tolerability for some time.
In any case, we should expect more companies to follow this strategy. There’s good tailwinds today, namely that (1) I&I is in the zeitgeist, and many targets are amenable to this approach, (2) the success of companies like Protagonist, DICE, and Morphic will inspire newcomers, and (3) chemistry technology is continuing to advance. I’m also hoping for is additional technologies that can be a broad-use platform, whether it’s an advance in macrocycle tech or a generalizable prodrug approach that can increase oral bioavailability.
Long live oral drugs. If you’re working in this space, please reach and and I’d love to chat.
Appendix
Table 1: list of oral drugs developed for antibody targets (non-comprehensive)
A few patterns emerge from examining this list:
The popular targets are often in large markets for drugs that require chronic use. I&I fits this bill in most cases, which is why we see several targets in that category
Macrocycles have been the modality of choice for many of these companies, but it’s also where we often see PK challenges come up during preclinical stages or in the clinic
Many of these molecules originated from a specific platform technology, such as DC-806 from DICE Therapeutics’ DEL platform and Morphic’s MORF-057 from their integrin platform.
Some molecules can take a long time to develop. For instance, Merck took 7 years to design their compound targeting PCSK9
Table 2: list of targets I’d love to see oral drugs developed for